|
|
|
|
|
|
|
Within a few days of weaning my “En” litter, I had a suspicion of what was wrong with our little orange collar puppy. A trip to the vet confirmed it and gave it a big name-- Persistent Right Aortic Arch. I recalled reading something about strictures of the esophagus from years past-- which prompted my suspicion and subsequent trip to the vet. But what exactly was PRAA, how was it treated, what was the prognosis? The year was 1999 and I sat for hours in front of my computer trying to find information to help my then-husband and I make an informed decision. But what I found most often did not concern itself with canines, and even that which I did find was very technical and not very helpful. Out of our experience comes this page—Angel’s page. A page where we will relate what I learned about PRAA and our own personal experience with corrective surgery, post-op care and long term care. My hope is that you will find the information you need to help you make an informed decision in deciding a course of action for your own puppy.
My “En” litter was whelped on September 1, 1999. Unfortunately, the last puppy was stillborn and the first puppy died a few hours later. This left a total of four puppies, two males and two females. The boys weighed in at 16 and 18 oz., the girls at 12 and 16 oz. As all the puppies were black and rust, we collared them with colored ric-rac to make identification faster. The smallest girl was graced with an orange collar.
|
|
|
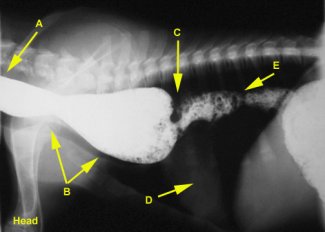
As luck would have it, the dam of the litter never got her milk in and I was left no option but to hand raise the puppies by tube feeding. During this time, orange collar steadily gained weight along with her litter mates, and by three weeks had practically caught up to her sister. But as usual, the puppies became more and more resistant to tube feeding with each passing day. By the time they were three weeks, it was necessary to start weaning them onto gruel. The first couple of days that they were on very soupy gruel went fine, albeit very messy! But as I started to increase the consistency of the gruel, a problem became apparent with the orange collar puppy. She would hungrily eat her portion, act distressed, frequently regurgitating her food, eat that down again and repeat the pattern. Sometimes this would repeat 4 or 5 times before she would keep the food down. At first I thought she perhaps was having an intolerance or food allergy, so I tried different food sources, but continued to have the same results—that’s when I started thinking stricture. During this weaning period, orange collar was losing weight, while her littermates were gaining fast on the gruel. It was time for action! I took orange collar to Roswell Animal Hospital and saw Lisa Hillier, DVM. I explained the puppy’s symptoms to her and she suggested a barium x-ray to confirm our suspicions. During this simple procedure, the puppy is given a small amount of thin, pasty food which has been mixed with a barium solution. Barium shows up very well on x-rays, and is used to diagnose a number of gastrointestinal disorders. After the puppy swallows the food an x-ray is taken to observe the track of the food down the esophagus. The hardest part of this procedure is timing the x-ray just right so that the barium mixture is in the part of the esophagus that you want to see. It took three x-rays to get the one we were looking for. In this x-ray, the barium mixture was seen clearly going easily down a normal sized esophagus, then just prior to the heart region was a dilation of the esophagus, followed by a portion of the esophagus looking like it was pinched off, followed by another open, clear and normal esophagus. Below is a barium x-ray of a typical PRAA puppy.
A- Barium mixture moving down
normal esophagus Image courtesy of Nathan Miller, DVM, University of Georgia School of Veterinarian Medicine, Athens, Georgia.
|
|
|
The very next day Angel was taken to the University of Georgia School of Veterinarian Medicine in Athens, Georgia as an emergency patient. Soft-tissue surgeon Nathan Miller, DVM saw Angel and discussed PRAA, the corrective surgery, post-op care and the long-term prognosis with me. PRAA is caused when the main vessel that transports blood away from the heart called the aorta, loops around the esophagus as the puppy is developing in the womb. This incorrect positioning of the aorta causes the esophagus to be strictured off—fluids typically pass the strictured area, but solids or semi-solid foods do not. These foods back up and pool in the esophagus in the area before the stricture, causing a dilation or ballooning of that area. A puppy with PRAA will regurgitate food repeatedly until it becomes liquefied sufficiently to pass the stricture. As was the case with Angel, it is most often during the course of weaning that PRAA is discovered. Each time a PRAA puppy regurgitates, it risks inhaling food matter back into the lungs (known as aspiration) causing infection and pneumonia. PRAA accounts for about seven percent of all congenital cardiovascular defects seen in dogs. It is potentially hereditary, but so far this has not been confirmed since there is so little population of affected dogs to study. At this point I should say that I was already an emotional wreck about this puppy. With every feeding, she had become more and more distressed as she tried to keep her food down, regurgitating often, gasping for air for 10-15 minutes at a time, frantic for food but losing weight. With each episode I was watching her waste away before me and I was left weeping, helpless to assist her and wondering if I was being cruel and selfish in trying to keep her alive. As Dr. Miller explained, since PRAA surgery is performed on very young puppies and in the critical area around the heart and lungs, she only had about a 80/20 chance of making through the surgery. But even after the surgery she would not be out of the woods, as aspiration of food into the lungs could cause pneumonia, which in her weakened condition could be life threatening. The long term outlook was not much better—she had a 50/50 chance of her esophagus returning to normal and hence leading a perfectly normal life. She also had a 50/50 chance of her esophagus remaining dilated and having to be fed special diets and fed elevated for life—not to mention the lifelong threat of food aspiration and subsequent pneumonia possibility. She would not live without the surgery, but the estimate for the surgery and subsequent hospital stay was $2,000 (luckily it turned out to be less)— a lot of money to spend on a pyramid of chances. But when talked to James (my husband at the time), he said it just didn’t seem right not to give her a chance despite the odds and the money. Despite all her hardships, she had always been bright eyed and a fighter. We counted on this as I signed the surgical release, said goodbye to her, and left the University hoping we had done the right thing. At four weeks and two days of age the little orange collar girl was operated on for two hours. Dr. Miller contacted me afterwards to give me the news that she had come through the surgery. Her constrictive aorta was surgically separated and repaired and her stomach was surgically and permanently attached to the left side of her abdominal wall- a necessary procedure to allow for an abdominal feeding tube. I was of course relieved, but knew that she had just cleared one of many hurdles. During her stay at UGA, she was the belle of the ball—being just a mere 2 pounds (her siblings back home were now at 4-5 pounds); she was carried around in the vet students’ pockets and constantly cared for. I knew that if she made it through this ordeal, she would be the most socialized puppy of the litter! Nightly I would get a call from her attending student to update us about her condition. The student would always start by saying, “This is so-n-so from UGA, just calling to let you know how Orange is doing.” It was quite ridiculous, so once she made it through the surgery, I decided to give her a call name. I hadn’t done so up to that point, because it is doubly hard to lose a puppy when it has a given name, and thus an identity. “Angel” was decided upon because she had an angelic expression, and because of the unseen spirit no doubt watching over her. Ten days after her surgery, James picked Angel up from the University. When I saw her I immediately broke down in tears—a mixture of joy that she was still alive and overwhelming despair over her appearance. At five and a half weeks, Angel barely registered 2 lbs., 5 oz, while her littermates were up to 6 lbs. Her left side had been shaved from stem to stern for the surgery, a surgical seam ran from her sternum almost up to her withers. A 4” feeding tube emerged from her side near her left flank- vet wrap was used to keep the loose end from flopping around and catching on something.
|
|
|
|
|
|
In this picture, you can see the surgical seam starting just behind her elbow and going up. The feeding tube emerges from her side; the capped feeding end appears just on top of her back, held in place by vet wrap. |
Post surgery, you can see the vast difference in size of Angel compared to her litter brother, Jackson. Only 2 ½ weeks earlier, Angel and Jackson were starting to be weaned and were within ounces of the same size and weight. |
|
Now that she was home, the real work began! To allow adequate time for her esophagus to heal from the trauma of the surgery, Angel had to be fed via her feeding tube. For the following week, we used a syringe to squirt food through her feeding tube. The tube had to be flushed out after each feeding, and the area cleaned and treated with ointment where the tube attached to her side. After that week, we returned to UGA to have her feeding tube removed.
The following five weeks were the hardest on us. During this phase, Angel had to be fed orally, by syringe, in an upright position. She then had to continue to be held in an upright position for another 20-30 minutes so gravity could help the food go down her esophagus properly. Because of the small amount of food she could be given at a time and the lower caloric value of the food, this had to be repeated every four hours around the clock.
|
|

Necessity is indeed the mother of invention! James came up with this very clever idea of using a fanny-pack to hold Angel during her feedings and to carry her upright afterwards. She was wrapped in a hand towel, placed in the bag, zipped up and the zipper held in place with a clothespin. This freed up our hands to work on other things while she was being held upright. Most often, Angel would fall asleep in this makeshift nest. |
|
|
What followed Angel’s return home was weeks upon weeks of continued struggles and hurdles to overcome. While Angel’s case is unique, anyone with a PRAA puppy who is considering the surgery should be aware of how vulnerable their puppy may be in its weakened condition. Just prior to her release from UGA, Angel was diagnosed with coccidia. Coccidia, single-celled organisms, are why campers are told to boil water taken from streams. It causes severe and bloody diarrhea and vomiting. In her weakened condition, this was the last thing that Angel needed. The coccidia was treated for two weeks with Albon. However, Angel’s symptoms of intermittent vomiting and diarrhea persisted. She would have 2 or 3 good days, followed by 2 or 3 really bad days. Overall, she was not gaining weight as she should have. This prompted many trips to the vet and various medications. Finally, at 11 weeks, she was OK’d to start eating from a bowl rather than by syringe (read further below about how she eats from a bowl). It was when we made this change in diet that her vomiting and diarrhea stopped—after all those weeks, it turned out that she had an intolerance to the prescription diet she had been placed on! At 11 weeks and weighing just 4 pounds (her siblings weighed 12-13 pounds at this point), I switched Angel to a meaty frozen food known for putting weight on dogs. While she loved it and did indeed gain weight quickly (2 ½ lbs. in one week—a 50% increase), after one week she began to display problems -- her front legs were becoming malformed. Another trip to the vet confirmed a diagnosis of rickets. Rickets is caused by a lack of nutrition, and the food I had chosen was believed by the vet to be the culprit (no doubt along with the prescription diet for which she had the intolerance). Later conversations with other breeders, who had also attempted to raise puppies on this food, revealed ricket-type symptoms in those puppies that subsequent changes of diet corrected. So I then changed her to a high quality dry kibble food (see below to see how it was prepared) which the other puppies in her litter had been raised on. Angel's littermates were thriving on the diet, however in less than 2 weeks Angel had sudden onset of extreme lameness, lethargy, vocal pain upon moving and fever of 104 degrees. Another trip to the vet and she was diagnosed with Hypertrophic Osteodystrophy (HOD). Unlike Pano (a wandering leg lameness common in puppies similar to growing pains in children), HOD can affect all the legs at once and can be so painful as to cause the dog to refuse to stand up at all. Dogs affected by HOD can fully recover, recover with permanent disability, or even die from high fevers. One of the believed triggers of HOD is a diet which is too high or too low in nutritional values. Once again, I switched Angel to another food, this time a nationally recognized dry kibble for large breed puppies (especially prepared of course). After 1½ weeks and two bouts of HOD, Angel was walking and playing normally. She was now 16 weeks old, weighed 12 pounds, and for the first time since I weaned the litter, we felt like Angel was finally out of the woods. Every time in the preceding weeks when she would have her “bad days” of relentless diarrhea and vomiting, and during her bouts with HOD, I would think to myself, “This is it. She’s not coming back this time. I’ll wake up in the morning and she’ll be gone.” Needless to say I was relieved, but emotionally and physically drained. All told, Angel’s vet bills from 3-16 weeks of age totaled over $2000, $1300+ of which was a direct result of the PRAA.
Since then a surgery for an umbilical hernia (a “hole” in the abdominal wall where the umbilical cord was) which had been put off for months, was performed successfully. She was also spayed with no problems at 8 mos. of age (besides the fact of her PRAA, Angel was not of show and/or breeding quality). After having been through so much already, to crop her ears seemed to add more insult to injury. Additionally, at this late age she would have had to have a very short ugly crop, so I opted to let her retain her natural look. This is a scan of a painting I commissioned of Angel in a field of clover showing her natural ears.
|
|
|
A LIFELONG COMMITMENT |
|
|
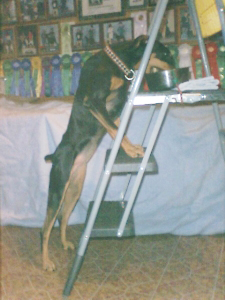
Angel’s esophagus dilation never corrected itself. Because of this she will always had to eat in an elevated position. This was accomplished by the use of a stepladder. At first a two-step stool was used, securing her food bowl to the top step while she stood with her front legs on the first step. When Angel outgrew the 2-step stool, a larger 3-step ladder was purchased for her feedings. This assured that gravity would help to carry food down her esophagus, bypassing the dilated area. Her food always had to be soupy in consistency to further aid in its passage. While on a dry kibble feed, this entailed double soaking the kibble and then adding even more water to it just prior to feeding. With so much moisture content, we had to be careful to take her outside frequently after feedings to empty her bladder.
I had to be very watchful of Angel and the things she played with. Stuffing from a toy, eaten grass, pieces of rawhide or bone would collect in her dilated esophagus area. A very small amount of any such foreign substance would block the passage of food down her esophagus. When this happened, she would regurgitate her meal, choking to get air in the meantime- this put her in a lifetime continued risk for aspiration pneumonia. After several attempts to eat and regurgitating, she usually would expel the foreign matter from her esophagus, but sometimes this did not happen for one to three days. On a few occasions she was not been able to expel the matter on her own, entailing yet more surgeries to remove it manually. Because Dobermans love to graze on grass, we had to keep a basket-type Greyhound muzzle with a protective guard on it, on Angel when she was outside. She could pant, bark and drink water with the muzzle, but it prevented her from grazing. While it looks bulky, Angel was accustomed to wearing the muzzle, and as she spent most of her time inside the house anyway, it really isn't a big deal to her.
|
|
|
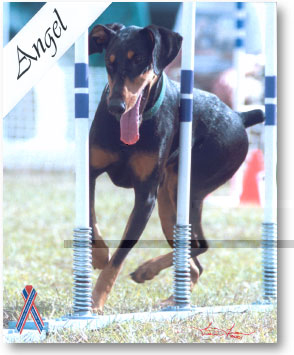
Despite her rough start, Angel grew healthy enough to compete in agility. Not only did she compete, but she went on to be one of the Top Twenty Dobermans in the country in agility for three years running. Due to her first four months of limited nutrition, Angel was very small for the Breed- topping out at 23-1/4” at the shoulder and weighing 48 pounds-- equivalent to a typical 6-8 mos old Doberman female puppy. The pictures below were taken of a novice, 13 month-old Angel competing at the 2000 DPCA Nationals. |
|
|
|
|
|
I hope Angel’s page is helpful to you if you have a PRAA puppy and are trying to decide to go ahead with surgery or not. The main things to keep in mind are 1) that the surgery is expensive; 2) the post-op care is intense, both physically and mentally; 3) surgical, post-op and total recovery are only about a 80/20 and 50/50 chance respectively; and 4) you must be willing to make a life-long commitment to special care. Of course, you must also factor in the life and love of your puppy, and if all goes well, a life long companionship. If you have any questions about Angle's experience, you are more than welcome to contact me.
|
|
|
|
|
|
ADAMAS
Enchanted Host MX, MXJ, WAC, CGC After a long and active life, Angel passed away one week shy of her 12th birthday. She is greatly missed. |
|
|
|
|
|
|
|





 Angel came home from UGA in October and with one
side totally shaved down. To keep her warm, old tube
socks were cut to fashion sweaters for her. In this
picture, she is sporting such a sock sweater and she has fallen
asleep with her head stuffed inside a shoe.
Angel came home from UGA in October and with one
side totally shaved down. To keep her warm, old tube
socks were cut to fashion sweaters for her. In this
picture, she is sporting such a sock sweater and she has fallen
asleep with her head stuffed inside a shoe.